Obstructive Sleep Apnea: A Clinical Review
Shanthi Priya K.1, Bandari G.2*, B L.3, Ramesh Goud S.4, Sriteja D.5, Smriti C.6
DOI: https://doi.org/10.17511/ijmrr.2022.i06.04
1 K Shanthi Priya, Reader, Department of Prosthodontics, MNR Dental College and Hospital, Sangareddy, Telangana, India.
2* Gayathri Bandari, Senior Resident, Department of Prosthodontics, Government Dental College and Hospital, Hyderabad, Telangana, India.
3 Lavanya B, Senior Lecturer, Department of Prosthodontics, AME’s Dental College & Hospital, Raichur, Karnataka, India.
4 S.V Ramesh Goud, Reader, Department of Orthodontics and Dentofacial orthopedics, Navodaya Dental College and Hospital, Raichur, Karnataka, India.
5 Dubhakunta Sriteja, Reader, Department of Orthodontics and Dentofacial orthopedics, Navodaya Dental College and Hospital, Raichur, Karnataka, India.
6 CH. Smriti, Postgraduate, Department of Prosthodontics, MNR Dental College and Hospital, Sangareddy, Telangana, India.
This article aims to provide a detailed description of obstructive sleep apnea regarding its signs and symptoms, the way it is diagnosed, the risk factors, management, and the role of dentists and oral appliances in treatment. Obstructive sleep apnea (OSA) is a potentially life-threatening disorder characterized by repeated collapse of the upper airway during sleep, with periodic cessation of breathing for more than ten seconds. Dental professionals have a unique doctor-patient relationship that can help them in recognizing the sleep disorder and co-managing the patients along with a physician or a sleep specialist. Oral appliance therapy is an important treatment modality for sleep apnea patients.
Keywords: Obstructive Sleep Apnea, Review, Oral Appliances
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Senior Resident, Department of Prosthodontics, Government Dental College and Hospital, Hyderabad, Telangana, India. Email:  |
K Shanthi Priya, Gayathri Bandari, Lavanya B, S.V Ramesh Goud, Dubhakunta Sriteja, CH. Smriti, Obstructive Sleep Apnea: A Clinical Review. Int J Med Res Rev. 2022;10(6):183-194. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1403 |
 |
 ©
© 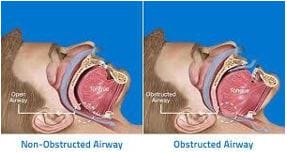 Figure 1: Difference showing Non-Obstructed and Obstructed airway
Figure 1: Difference showing Non-Obstructed and Obstructed airway Figure 2: Risks Of Obstructive Sleep Apnea
Figure 2: Risks Of Obstructive Sleep Apnea

 Figure: 5 Tongue retaining devices ( TRD)
Figure: 5 Tongue retaining devices ( TRD)  Figure 6: Mandibular repositioning appliance
Figure 6: Mandibular repositioning appliance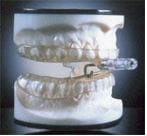 Figure 7: Thornton Adjustable Positioner
Figure 7: Thornton Adjustable Positioner Figure 8: Tongue Stabilizing Device
Figure 8: Tongue Stabilizing Device