Tubercular Osteomyelitis of Jaw: A Rare Case Report
Prashant D.1, Prashant V.2*
DOI: https://doi.org/10.17511/ijmrr.2022.i06.01
1 Dolly Prashant, Assistant Professor, Department of Pathology, Govt Dental College, Raipur, Chhattisgarh, India.
2* Viplav Prashant, Associate Professor, Department of Biochemistry, Govt Dental College, Raipur, Chhattisgarh, India.
Tubercular (TB) osteomyelitis of the mandible is a rare and uncommon clinical condition. The clinical appearance of tubercular infection of the temporomandibular joint (TMJ) comprises nonspecific features resembling osteomyelitis, arthritis, or any other kind of chronic joint disease. At times, localized painful swelling of the jaw may be the only manifestation. The presented case is of osteomyelitis of the jaw in a 14-year-old girl patient for whom TB was later suspected.
Keywords: Tubercular Osteomyelitis, Localized Jaw Swelling, Temporomandibular Joint
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, Department of Biochemistry, Govt Dental College, Raipur, Chhattisgarh, India. Email:  |
Dolly Prashant, Viplav Prashant, Tubercular Osteomyelitis of Jaw: A Rare Case Report. Int J Med Res Rev. 2022;10(6):166-170. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1402 |
 |
 ©
©  Figure 1: Examination of the oral cavity
Figure 1: Examination of the oral cavity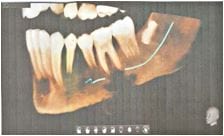
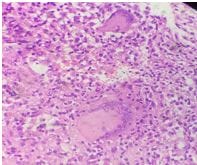 Figure 3c: Area of necrosis with Langhans giant cells (40x view)
Figure 3c: Area of necrosis with Langhans giant cells (40x view)