A study to determine calorie and protein intake in adolescent school girls of Indore city, M.P., India
Solanki S.1, Solanki M.2*
DOI: https://doi.org/10.17511/ijmrr.2021.i06.10
1 Sunita Solanki, Associate Professor, Department of Physiology, M.G.M. Medical College, Indore, Madhya Pradesh, India.
2* Mahendra Solanki, Associate Professor, Department of Orthopaedics, M.G.M. Medical College and Associated Hospitals, Indore, Madhya Pradesh, India.
Introduction: Adolescence is a significant period of human growth and maturation. This period of rapid growth requires a well-balanced diet. An inadequate diet and unfavourable environment adversely influence the growth resulting in short stature and low lean body mass. Not much attention has been paid to adolescents by nutrition-related programmes. Hence, this study was planned to assess the dietary intake of adolescent girls. Method: This was a cross-sectional study conducted in five schools in urban areas of Indore city. The study group included 400 school girls of age 11 to 18 years. After taking written informed consent from the parents, data was collected on personal information, dietary intake and socioeconomic status. Anthropometric measurements were done, and data were analyzed. Results: The calorie intake in this study ranged from 69% to 86% of R.D.A. Mean protein intake ranged from 71.5% to 73.7% of R.D.A., and mean iron intake ranged from 50% to 71.4% R.D.A. All the girls were consuming an inadequate amount of calories, proteins and iron. Conclusion: All the adolescent girls in this study had low intakes of calories, iron and protein, which is comparable to that found in other Indian studies.
Keywords: Adolescent girls, Calorie intake, Protein intake, Iron intake, Indore
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, Department of Orthopaedics, M.G.M. Medical College and Associated Hospitals, Indore, Madhya Pradesh, India. Email:  |
Sunita Solanki, Mahendra Solanki, A study to determine calorie and protein intake in adolescent school girls of Indore city, M.P., India. Int J Med Res Rev. 2021;9(6):406-411. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1386 |
 |
 ©
© 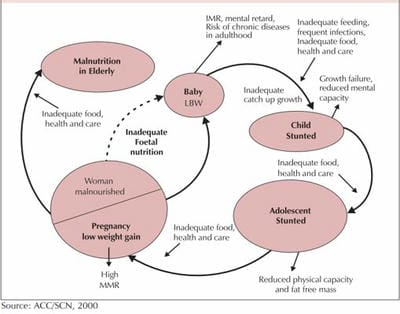 Figure 1: Nutrition throughout the life cycle.
Figure 1: Nutrition throughout the life cycle.