Parasitic Hypoproteinemia: A Diagnostic Dilemma in an Immunocompetent Patient
Maitra S.1*, Pal D.2, Ray K.3, Adnan Yusuf S.4
DOI: https://doi.org/10.17511/ijmrr.2022.i02.05
1* Somnath Maitra, Associate Professor, Department of General Medicine, JIMSH, Budge, Kolkata, West Bengal, India.
2 Debes Pal, Associate Professor, Department of Pathology, JIMSH, Budge, Kolkata, West Bengal, India.
3 Koushik Ray, Assistant Professor, Department of Anatomy, JIMSH, Budge, Kolkata, West Bengal, India.
4 Sk Adnan Yusuf, Senior Resident, Department of General Medicine, JIMSH, Budge, Kolkata, West Bengal, India.
Strongyloidiasis is caused by a nematode helminth which causes multisystem involvement with signs and symptoms related to the gastrointestinal, pulmonary, dermatological and nervous systems. The index case discussed here presented with edema, hypoalbuminemia, malnutrition and anemia with urease positive duodenal ulcer. Duodenal biopsy suggested malabsorption, and strongyloidiasis was detected in the biopsy, which clinched the diagnosis and treatment was given with ivermectin, after which the patient improved and responded to treatment. The importance lies in the fact that parasitic infections may cause malabsorption even in immunocompetent patients, which is a rare entity but must not be missed as it responds to treatment promptly, which is cheap and effective.
Keywords: Strongyloidiasis, hypoalbuminemia, malabsorption, anemia
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, Department of General Medicine, JIMSH, Budge, Kolkata, West Bengal, India. Email:  |
Somnath Maitra, Debes Pal, Koushik Ray, Sk Adnan Yusuf, Parasitic Hypoproteinemia: A Diagnostic Dilemma in an Immunocompetent Patient. Int J Med Res Rev. 2022;10(2):81-84. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1379 |
 |
 ©
© 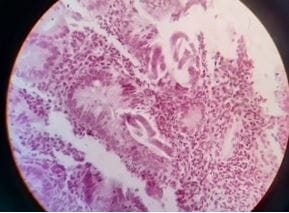 Figure 1: Strongyloides in duodenal biopsy
Figure 1: Strongyloides in duodenal biopsy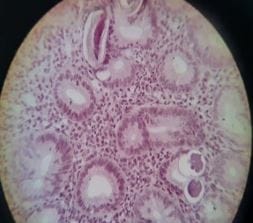 Figure 2: Strongyloides in duodenal biopsy
Figure 2: Strongyloides in duodenal biopsy Figure 3: Koilonychia and leukonychia
Figure 3: Koilonychia and leukonychia