Impact on Undefined Normal Tissue by using the different combination of Normal Tissue Objective and Dose Control Ring in IMRT Plans for Cervix cancer
Muthukumar S.1, Navitha S.2*, Nigam J.3, Silambarasan N.4, Kumar P.5
DOI: https://doi.org/10.17511/ijmrr.2022.i02.03
1 S Muthukumar, Intern Medical Physicist, Department of Radiation Oncology, SRMS Institute of Medical Sciences, Bareilly, U.P, India.
2* S Navitha, Medical Physicist, Department of Radiation Oncology, SRMS Institute of Medical Sciences, Bareilly, U.P, India.
3 Jitendra Nigam, Medical Physicist, Department of Radiation Oncology, SRMS Institute of Medical Sciences, Bareilly, U.P, India.
4 NS Silambarasan, Medical Physicist, Department of Radiation Oncology, SRMS Institute of Medical Sciences, Bareilly, U.P, India.
5 Piyush Kumar, Professor and Head, Department of Radiation Oncology, SRMS Institute of Medical Sciences, Bareilly, U.P, India.
Introduction: Normal tissue objective is tool used in inverse planning of Intensity Modulated Radiation Therapy reduce dose spreading surrounding normal tissues. Multitude of potential NTO setting combinations challenges optimal NTO tunning. Aim and Objective: Find impact on Undefined Normal Tissue (UNT) by using different combinations of NTO and DCR in IMRT Plans for Cervical cancer plans. Materials and Methods: Our sample consists of 30 patients with similar treatment prescription doses. Varian Eclipse Treatment Planning System Version13.6 was used in study. 5 different plans were created each patient.Every plan beam energy, several beams, Beam angle, Optimization algorithm - Photon optimizer (PO), Calculation algorithm – Anisotropic analytic algorithm, evaluation methods were maintained constant. 5 plans were different only in optimization process. Before generating plans DCR thickness 1.0 cm and 0.5 cm away from Planning Target Volume was created. Plan with different combinations between NTO, DCR were A. Without NTO, B. Automatic NTO, C. Manual NTO, D. Automatic NTO + DCR, E. Manual NTO + DCR generated. Plan quality was evaluated by comparing PTV: Conformity Index (CI), Homogeneity Index, OAR Doses and mean dose to UNT. Results: HI was better without NTO plans compared to all other plans. CI and OAR doses show significant difference in Manual NTO along with DCR plans. Conclusion: Study shows manual NTO + Dose Control Ring gives better plan quality terms PTV coverage, less dose to Undefined Normal Tissue by maintaining Organ at Risk dose within tolerance limits.
Keywords: Intensity Modulated Radiation Therapy, Normal tissue objective, Undefined Normal Tissue, Radiotherapy, Cervix Cancer
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Medical Physicist, Department of Radiation Oncology, SRMS Institute of Medical Sciences, Bareilly, U.P, India. Email:  |
S Muthukumar, S Navitha, Jitendra Nigam, NS Silambarasan, Piyush Kumar, Impact on Undefined Normal Tissue by using the different combination of Normal Tissue Objective and Dose Control Ring in IMRT Plans for Cervix cancer. Int J Med Res Rev. 2022;10(2):69-74. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1376 |
 |
 ©
© 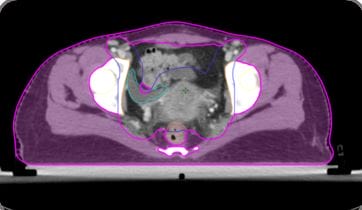 Figure 1: Undefined Normal Tissue (UNT)
Figure 1: Undefined Normal Tissue (UNT)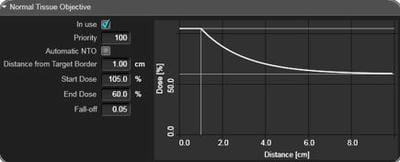 Figure 2: Normal Tissue Objective (NTO)
Figure 2: Normal Tissue Objective (NTO)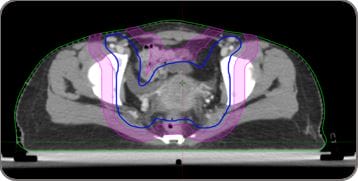 Figure 3: Dose Control Ring (DCR)
Figure 3: Dose Control Ring (DCR)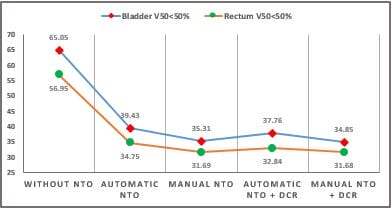 Graph 1: Comparison of Urinary Bladder (V50<50%) and Rectum (V50<50%) for all the plans. Here we indicated the mean values of the 30 patients, for each type of planning.
Graph 1: Comparison of Urinary Bladder (V50<50%) and Rectum (V50<50%) for all the plans. Here we indicated the mean values of the 30 patients, for each type of planning.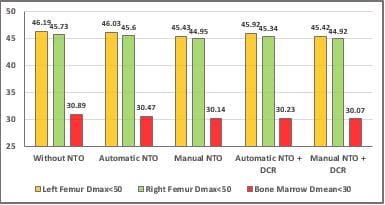 Graph 2: Comparison of Left Femur (DMax<50Gy) for all the plans. Here we indicated the mean values of the 30 patients, for each type of planning.
Graph 2: Comparison of Left Femur (DMax<50Gy) for all the plans. Here we indicated the mean values of the 30 patients, for each type of planning.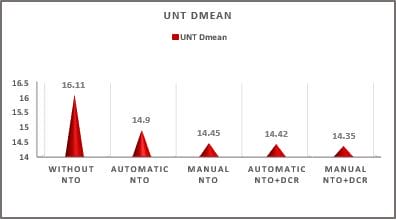 Graph 3: Comparison of Undefined Normal Tissue (DMean) for all the plans. Here we indicated the mean values of the 30 patients, for each type of planning.
Graph 3: Comparison of Undefined Normal Tissue (DMean) for all the plans. Here we indicated the mean values of the 30 patients, for each type of planning.