Laboratory profile of COVID-19 Patients at the time of admission
Basak I.1, Krishnamurthy V.2*
DOI: https://doi.org/10.17511/ijmrr.2022.i02.04
1 Indrakshi Basak, Postgraduate, pathology, JSS Medical College, JSS Academy of Higher Education and Research, Mysuru, Karnataka, India.
2* Vani Krishnamurthy, Associate professor, Pathology, JSS Medical College, JSS Academy of Higher Education and Research, Mysuru, Karnataka, India.
Background: COVID-19 is a recent pandemic, the complete picture of which is yet to be described. Recent advances in the treatment and improved outcomes have been contributed mainly by knowing the pathological and biochemical status of the patients. Further improvement in understanding this disease at all levels will help in formulating appropriate management plans. Objective: To describe the various biochemical and haematological parameters of COVID – 19 positive patients at the time of admission to the hospital for treatment. Method: We analysed the biochemical and haematological parameters of 100 COVID patients admitted to our hospital from June 2020 to September 2020. Results: 60.6% of our subjects were between 40 and 70 Years. 74.7% of the cases were males. Fever and cough were the most frequent complaints and 49. 5% of them had pneumonia at the time of admission. 19% of the patients needed ICU management. The most common haematological abnormality was lymphopenia seen in 79.9% followed by Eosinopenia seen in 46.5%. Reactive lymphocytes were seen in the majority of the patients (84 %). Toxic granules in the neutrophils, fragmented RBCs and significant left shift of neutrophils are found in small proportions. CRP was elevated in 92% of our patients, followed by elevated Ferritin in 78.2%. D-Dimer was elevated in 44.4% of the patients. Conclusion: The majority of Covid patients at presentation have deranged coagulation and increased D-Dimer. Lymphopenia is the most common haematological abnormality.
Keywords: COVID-19, Haematological parameters, Lymphopenia, Eosinopenia, D-dimer
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate professor, Pathology, JSS Medical College, JSS Academy of Higher Education and Research, Mysuru, Karnataka, India. Email:  |
Indrakshi Basak, Vani Krishnamurthy, Laboratory profile of COVID-19 Patients at the time of admission. Int J Med Res Rev. 2022;10(2):75-80. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1371 |
 |
 ©
© 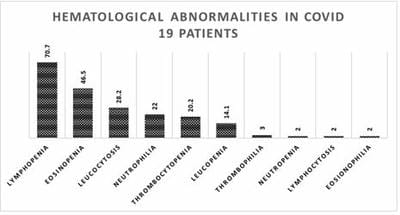 Figure 1: Haematological abnormalities (excluding RBC) seen in COVID -19 patients in the order of frequency
Figure 1: Haematological abnormalities (excluding RBC) seen in COVID -19 patients in the order of frequency