Enteric Encephalopathy associated with reversible ECG changes: A Diagnostic Dilemma
Maitra S.1*, Yusuf S.2, Ray K.3
DOI: https://doi.org/10.17511/ijmrr.2022.i01.08
1* Somnath Maitra, Associate Professor, General Medicine, Jagannath Gupta Institute of Medical Sciences and Hospital, Budge Budge, Kolkata, West Bengal, India.
2 Sk Adnan Yusuf, Senior Resident, General Medicine, Jagannath Gupta Institute of Medical Sciences and Hospital, Budge Budge, Kolkata, West Bengal, India.
3 Koushik Ray, Assistant Professor, Anatomy, Jagannath Gupta Institute of Medical Sciences and Hospital, Budge Budge, Kolkata, West Bengal, India.
Enteric fever is common in India. It presents with various clinical manifestations. Encephalopathy and ECG changes are indicators of prognosis. Persistent ECG changes indicate a poor prognosis. The pathogenesis of encephalopathy is unclear though prostaglandins and free oxygen species may be implicated in the prognosis and justifies the use of steroids in enteric encephalopathy with antibiotics. The case presented here presented with encephalopathy and ECG changes which reversed following antibiotic and steroid therapy. The importance of the case lies in the fact that typhoid should not be missed in the diagnosis of encephalopathy and ECG should be done in all cases of enteric fever to determine the prognosis.
Keywords: Enteric fever, Encephalopathy, ECG changes, Prognosis
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, General Medicine, Jagannath Gupta Institute of Medical Sciences and Hospital, Budge Budge, Kolkata, West Bengal, India. Email:  |
Somnath Maitra, Sk Adnan Yusuf, Koushik Ray, Enteric Encephalopathy associated with reversible ECG changes: A Diagnostic Dilemma. Int J Med Res Rev. 2022;10(1):53-56. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1369 |
 |
 ©
© 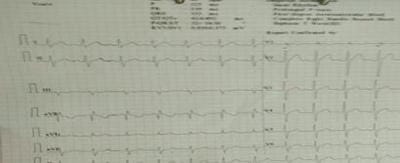 Figure 1: Showing ECG changes of Enteric Fever with RBBB,First degree AV block and Biphasic T waves.
Figure 1: Showing ECG changes of Enteric Fever with RBBB,First degree AV block and Biphasic T waves.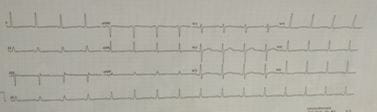 Figure 2: Showing ECG changes which reversed following recovery from Enteric Fever.
Figure 2: Showing ECG changes which reversed following recovery from Enteric Fever.