The pattern of Parental Handling in Children with Emotional and Behavioural Disorders - A Cross-Sectional Study
Raju R.1, Roy G M.2*
DOI: https://doi.org/10.17511/ijmrr.2023.i02.01
1 Rajani Raju, Department of Psychiatry, Government Medical College Trivandrum, Kerala, India.
2* Mohan Roy G, Department of Psychiatry, Government Medical College Trivandrum, Kerala, India.
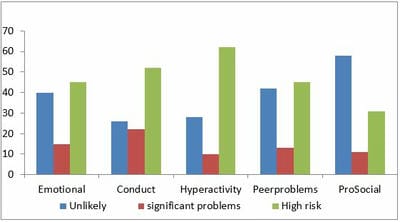
Introduction: This study is to determine patterns of parental handling in children with emotional and behavioural disorders, and to determine the correlation of parental handling patterns to the child’s behavioural and emotional symptoms. Methods: A cross-sectional study was conducted over one year among the parents of children and adolescents aged 4 to 17 years diagnosed with emotional and behavioural disorders and consulting a tertiary care centre in Kerala, South India, for the first time. Results: Most parents showed low care and low control patterns, while a majority of the children were at high risk for clinically significant problems. Approximately 62% of the children were at high risk due to hyperactivity/inattention, 45% for issues with peers, and 33% for poor prosocial behavior. There was a significant negative correlation between the control and conduct symptoms (ρ=-.232, p=0.020) and between control and hyperactivity (ρ-.221, p=0.027). A significant positive correlation was observed between emotional symptoms and the educational status of the parent (ρ=.265, p=0.008), and between peer problems and the age of the child (ρ=.232, p=0.020). There was also a significant correlation between externalising disorders and control scores. Conclusion: The population was found to predominantly have low care and low control patterns, i.e., less optimal parenting styles. Parental control was found to positively influence conduct symptoms and hyperactivity symptoms. There was no relation between socio-demographic factors and the pattern of parental handling or between parental handling patterns and other emotional and behavioural symptoms in the child.
Keywords: Parental handling, Pattern, Emotional and Behavioural Disorders, Children
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , , Department of Psychiatry, Government Medical College Trivandrum, , Kerala, India. Email:  |
Rajani Raju, Mohan Roy G, The pattern of Parental Handling in Children with Emotional and Behavioural Disorders - A Cross-Sectional Study. Int J Med Res Rev. 2023;11(2):28-34. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1364 |
 |
 ©
©