Volumetric and dosimetric effects of different slice thickness in radiotherapy planning Computed Tomography for Head and Neck cancer
Fazilathunnisa J.1, Navitha S.2*, Nigam J.3, Silambarasan N.4, Kumar P.5
DOI: https://doi.org/10.17511/ijmrr.2022.i02.01
1 J Fazilathunnisa, Intern, Medical Physicist, Department of Radiation Oncology, SRMS Institute of Medical Sciences, Bareilly, UP, India.
2* S Navitha, Medical Physicist, Department of Radiation Oncology, SRMS Institute of Medical Sciences, Bareilly, UP, India.
3 Jitendra Nigam, Medical Physicist, Department of Radiation Oncology, SRMS Institute of Medical Sciences, Bareilly, UP, India.
4 NS Silambarasan, Medical Physicist, Department of Radiation Oncology, SRMS Institute of Medical Sciences, Bareilly, UP, India.
5 Piyush Kumar, Professor & Head, Department of Radiation Oncology, SRMS Institute of Medical Sciences, Bareilly, UP, India.
Introduction: Accurate estimation of target and Organ at Risk Volume is required to ensure treatment efficacy and minimal normal tissue toxicity in radiotherapy planning. Computed Tomography slice thickness plays a vital role in volume estimation. It highly impacts smaller volume organs such as 1-3cm3.Materials and Methods: CT datasets of 20 head and neck cancer patients were recruited for this study in each CT data three CT series with a slice thickness of 1.5mm, 3mm and 5mm were imported to the TPS. Eclipse TPS of version 13.6 was used for delineation and treatment planning. Results: The variability of volumes with CT slice thickness was significant, especially for small volume structures. The maximum volume error of 63% was found in >3cc volume structures with 5mm slice thickness. Whereas in larger volume structures the differences were observed 2%in terms of volume and mean dose. And in terms of homogeneity and conformity, there is no significant difference was found. Conclusion: This study concludes that for head and neck cancer which has many smaller volume structures 1.5mm slice thickness will accurately estimate the volume which is clinically useful for OAR near the PTV.
Keywords: Radiotherapy, IMRT, Head and Neck cancer, Slice thickness, Small volume organs
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Medical Physicist, Department of Radiation Oncology, SRMS Institute of Medical Sciences, Bareilly, UP, India. Email:  |
J Fazilathunnisa, S Navitha, Jitendra Nigam, NS Silambarasan, Piyush Kumar, Volumetric and dosimetric effects of different slice thickness in radiotherapy planning Computed Tomography for Head and Neck cancer. Int J Med Res Rev. 2022;10(2):57-62. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1362 |
 |
 ©
© 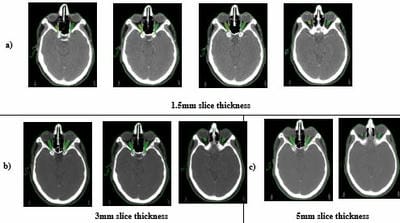 Figure 1: Contour of optic nerve in different CT slice thickness.
Figure 1: Contour of optic nerve in different CT slice thickness.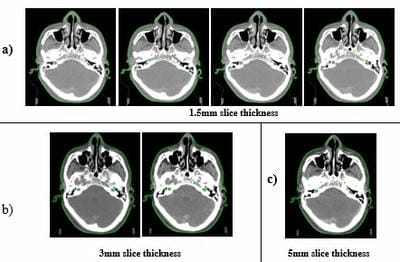 Figure 2: Contour of cochlea.
Figure 2: Contour of cochlea.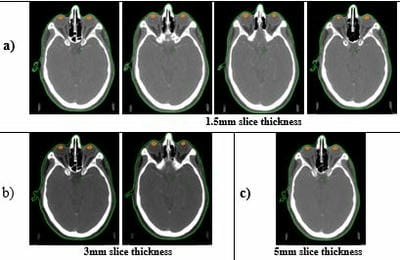 Figure 3: Contour of the lens.
Figure 3: Contour of the lens.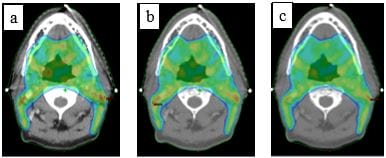 Figure 4: Dose color wash of 95% dose coverage to the Planning target volume: a) 1.5mm b) 3mm and c) 5mm slice thickness.
Figure 4: Dose color wash of 95% dose coverage to the Planning target volume: a) 1.5mm b) 3mm and c) 5mm slice thickness.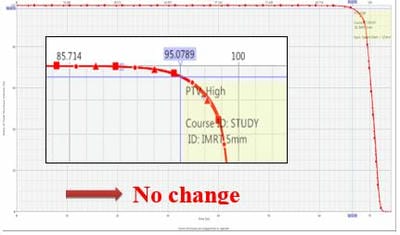 Figure 5: Dose-volume Histogram curve of planning target volume with 1.5mm, 3mm and 5mm slice thicknesses.
Figure 5: Dose-volume Histogram curve of planning target volume with 1.5mm, 3mm and 5mm slice thicknesses.