To Study the Computed Tomography Temporal Bone Findings in Patients with Chronic Suppurative Otitis Media
Mandal P.1, Vasanthan R.2*, Kumar K.3, Prabu V.4, Govardhanan .5
DOI: https://doi.org/10.17511/ijmrr.2022.i01.02
1 Priyanka Mandal, Senior Resident, Department of Radio-Diagnosis, Sri Venkateshwaraa MCH and Research Center, Puducherry, , India.
2* Ratna Vasanthan, Associate Professor, Department of Radio-Diagnosis, Sri Venkateshwaraa MCH and Research Center, Puducherry, , India.
3 Krishna Kumar, Professor, Department of Radio-Diagnosis, Sri Venkateshwaraa MCH and Research Center, Puducherry, , India.
4 Velayutham Prabu, Professor, Department of Otorhinolaryngology, Sri Venkateshwaraa MCH and Research Center, Puducherry, , India.
5 Govardhanan, Professor, Department of Radio-Diagnosis, Sri Venkateshwaraa MCH and Research Center, Puducherry, , India.
Background: Chronic suppurative otitis media is a chronic inflammation of middle ear cleft. It can present with discharging ear and decreased hearing. Diagnosis is mostly on clinical examination with an otoscope or otoendoscope. Our study was undertaken to evaluate role of computed tomography in defining extent and severity of various pathological changes occurring in temporal bone in case of chronic suppurative otitis media. Materials and Methods: Current study was a prospective cross-sectional study was conducted in Sri Venkateshwaraa Medical College and Research Center, Ariyur, Pondicherry from January 2019 to May 2020. Study included 60 patients clinically diagnosed with a chronic middle ear infection and who were referred to Department of Radiodiagnosis and Imaging for an HRCT scan of temporal bone. All obtained data were entered in Microsoft Excel and analyzed with SPSS 23.0 software. Results: In our study, a total number of 60 patients were involved. Youngest patient was aged 7 years and oldest patient’s age was 63 years. Majority (28.33%) of patients were aged between 21-30 years followed by 26.67% in 11-20 years age group. Our study found site and extent of involvement of middle ear and mastoid air cell system as follows: protympanum (20.00%); meso-tympanum (26.67%); posterior tympanum (30.00%); epitympanum (60.00%); hypo-tympanum (25.00%); peri-labyrinthine cells (1.67%); aditus (53.33%); antrum (40.00%); mastoid air cells (58.33%). Conclusion: HRCT scan is a unique method to detect early cholesteatoma and also to detect cholesteatoma in hidden areas.
Keywords: Chronic suppurative otitis media; High Resolution Computed tomography; Cholesteatoma
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, Department of Radio-Diagnosis, Sri Venkateshwaraa MCH and Research Center, Puducherry, , India. Email:  |
Priyanka Mandal, Ratna Vasanthan, Krishna Kumar, Velayutham Prabu, Govardhanan, To Study the Computed Tomography Temporal Bone Findings in Patients with Chronic Suppurative Otitis Media. Int J Med Res Rev. 2022;10(1):10-16. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1360 |
 |
 ©
© 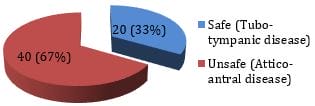 Figure 1: Distribution of the impression of HRCT findings regarding CSOM type.
Figure 1: Distribution of the impression of HRCT findings regarding CSOM type. Figure 2: Distribution of the HRCT findings of temporal bone regarding mastoid pneumatization (n=60).
Figure 2: Distribution of the HRCT findings of temporal bone regarding mastoid pneumatization (n=60).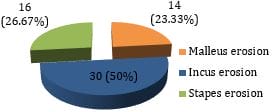 Figure 3: Distribution of the HRCT findings regarding ossicular involvement.
Figure 3: Distribution of the HRCT findings regarding ossicular involvement.