First Trimester Screening by Ultrasonographic Markers for Prediction of Pre-eclampsia
Pandey S.1, Gupta V.2, Shukla R.3, Gupta D.4*
DOI: https://doi.org/10.17511/ijmrr.2021.i06.04
1 Seema Pandey, Associate Professor, Department of Radiodiagnosis, MLN Medical College, Prayagraj, U.P, India.
2 Veena Gupta, Professor, Department of Obstetrics and Gynaecology, MLN Medical College, Prayagraj, U.P, India.
3 Rakesh Kumar Shukla, Assistant Professor, Anatomy, MVASMC, Mirzapur, U.P, India.
4* Divya Gupta, Resident, Department of Obstetrics and Gynaecology, MLN Medical College, Prayagraj, U.P, India.
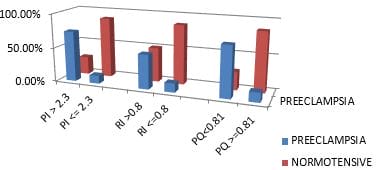
Aim: To correlate the association of ultrasonographic markers in antenatal patients with subsequent development of pre-eclampsia. Material Method: 131 pregnant women in the first trimester of pregnancy were investigated for their uterine artery Doppler and placental volume. These patients were followed up till the term for the development of pre-eclampsia. Results: Out of 131 antenatal cases, 20.61% developed pre-eclampsia. Uterine artery Pulsatility index >95th percentile (>2.3) with mean 2.08±0.43 (p-value 0.0001) predicted pre-eclampsia with a sensitivity of 51.85% with a specificity of 95.19%. Similarly, the Resistance index of the Uterine artery >95th percentile (>0.8) with a mean 0.771±0.084 (p-value 0.018) predicted pre-eclampsia with a sensitivity of 48.15% and specificity of 87.50%. Placental Quotient <10th percentile (<0.81) with mean 0.89 (p-value 0.0001) predicted pre-eclampsia with a sensitivity of 40.74% and specificity of 96%. On combining all three ultrasonographic parameters, the sensitivity for prediction of pre-eclampsia was increased to 70.37% with a specificity of 86.54% with PPV of 36.74% and NPV of 96.34%. Conclusion: Maternal ultrasonographic markers like Uterine artery PI, RI, Placental Quotient levels vary between normal pregnancies and those that subsequently developed pre-eclampsia. Thus our study concludes that first-trimester screening with ultrasonographic markers has high sensitivity, specificity and negative predictive value in detecting pre-eclampsia.
Keywords: Preeclampsia, Pulsatility index, Ultrasonography
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Resident, Department of Obstetrics and Gynaecology, MLN Medical College, Prayagraj, U.P, India. Email:  |
Seema Pandey, Veena Gupta, Rakesh Kumar Shukla, Divya Gupta, First Trimester Screening by Ultrasonographic Markers for Prediction of Pre-eclampsia. Int J Med Res Rev. 2021;9(6):374-378. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1357 |
 |
 ©
©