A prospective, observational study of Cosmelite NextTM therapy to evaluate the efficacy and safety of a novel plant-derived combination in the treatment of Melasma at dermatological centres in Hyderabad
Parthasaradhi A.1*, Arragudla V.2, Mamidala H.3
DOI: https://doi.org/10.17511/ijmrr.2021.i05.10
1* Anchala Parthasaradhi, Director, Dermatology, Anchala skin institute, Hyderabad, Telangana, India.
2 Vikram Kumar Arragudla, Dermatologist, Dermatology, Anchala skin institute, Hyderabad, Telangana, India.
3 Himabindu Mamidala, Dermatologist, Dermatology, Anchala skin institute, Hyderabad, Telangana, India.
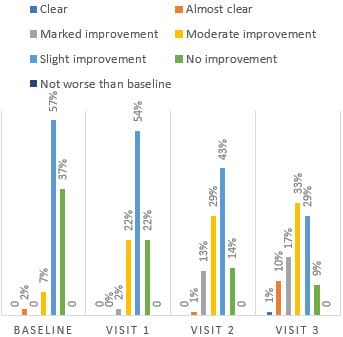
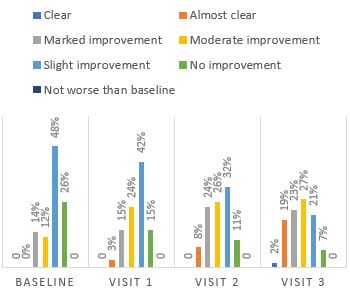
Background and objectives: Melasma, an acquired condition of skin hyperpigmentation, is a difficult condition to treat. This study was conducted to evaluate the efficacy and safety of a novel plant-derived combination for Melasma, Cosmelite NextTM, containing a combination of silymarin (0.7%), soy Isoflavones (0.25%), pTerowhite (0.10%), kojic acid (2%), ascorbic acid (1%), niacinamide (4%) and mandelic acid (3%). Material and Methods: This was an open-label, single-arm, prospective, multi-centre observational study at dermatological centres in Hyderabad, India. Patients diagnosed with Melasma of either gender and skin type consistent with Fitzpatrick phototypes I-IV categories were enrolled across Hyderabad, India. Outcomes included melasma area and severity index (MASI) score, lesion score, physician's global assessment (PGA) and patient's global assessment score. Results: In terms of the primary variable, the change from baseline score to 12 weeks in MASI was statistically significant (mean difference 1.46 (95% CI 1.39–1.52); p=0.001), and the decreasing trend was observed from week four onwards. Lesion scores also decreased from the baseline to week 12, with a mean difference of 1.46 (95% CI 1.39–1.52; p=0.001). At the end of the study period, 91% of the patients showed some improvement in the PGA, whereas 93% showed improvement in the patients' global assessment score. Conclusion: Cosmelite NextTM was safe and efficacious, and the improvements in assessment scores were seen as early as four weeks. The novel combination could be an effective alternative to conventional treatments such as hydroxyquinone, retinoids and steroid preparations.
Keywords: Melasma, Silymarin, Soy Isoflavones, Kojic acid, Ascorbic acid, Mandelic acid
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Director, Dermatology, Anchala skin institute, Hyderabad, Telangana, India. Email:  |
Anchala Parthasaradhi, Vikram Kumar Arragudla, Himabindu Mamidala, A prospective, observational study of Cosmelite NextTM therapy to evaluate the efficacy and safety of a novel plant-derived combination in the treatment of Melasma at dermatological centres in Hyderabad. Int J Med Res Rev. 2021;9(5):343-350. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1344 |
 |
 ©
©