A rare presentation of hyperhomocysteinemia and folate deficiency as CSVT in young male
Mallikarjun S.1*, Hassan K.2, Prahlad B.3, Puranic B.4
DOI: https://doi.org/10.17511/ijmrr.2021.i06.09
1* Shetty Mallikarjun, Post Graduate, Department of General Medicine, Shadan Institute of Medical Sciences, Hyderabad, Telangana, India .
2 Kamal Hassan, Associate professor, Department of General Medicine, Shadan Institute of Medical Sciences, Hyderabad, Telangana, India.
3 B Prahlad, HOD and Professor, Department of General Medicine, Shadan Institute of Medical Sciences, Hyderabad, Telangana, India.
4 Basawaraj Puranic, Professor, Department of General Medicine, Shadan Institute of Medical Sciences, Hyderabad, Telangana, India.
Introduction: Cerebral sinus venous thrombosis (CSVT) is a relatively rare, potentially fatal neurological condition that can be frequently overlooked due to its vague nature and its varied spectrum of clinical presentation. It’s a multifactorial condition with gender-related specific causes. It’s a rare form of venous thromboembolism representing almost 0.5-3 % of all types of stroke, affecting predominantly younger people, and females three times more commonly affected than males. Incidents in adults are 3- 4 million. The diagnosis of CSVT is becoming easier now days due to advanced neuroimaging techniques. Abnormality in the thrombophilic profile is associated with enhanced risk of CSVT. It has varied etiologies such as the Hypercoagulable States (inherited) that is hyperhomocysteinemia, protein C and protein S deficiency, Antithrombin-III deficiency, Factor V leiden mutations, autoimmune causes. Other acquired causes like CNS infection, trauma, dehydration, pregnancy, substances abuse and oral contraceptives.
Keywords: Hyperhomocysteinemia, Cerebral sinus venous thrombosis (CSVT)
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Post Graduate, Department of General Medicine, Shadan Institute of Medical Sciences, Hyderabad, Telangana, India . Email:  |
Shetty Mallikarjun, Kamal Hassan, B Prahlad, Basawaraj Puranic, A rare presentation of hyperhomocysteinemia and folate deficiency as CSVT in young male. Int J Med Res Rev. 2021;9(6):403-405. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1343 |
 |
 ©
© 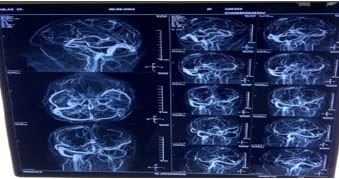 Fig 1: MRI Brain showing Non visualization of Sinus.
Fig 1: MRI Brain showing Non visualization of Sinus.