Is there any association between vitamin D deficiency and anti-thyroid peroxidase positive hypothyroidism: A cross-sectional study
Shankar M.1, Singh M.2*
DOI: https://doi.org/10.17511/ijmrr.2020.i04.02
1 Meenakshi Shankar, Senior Resident, , Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, , India.
2* Mukul Singh, Professor, , Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, , India.
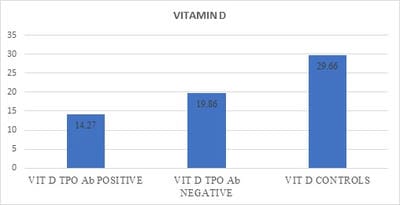
Background: Vitamin D deficiency is prevalent worldwide and it is believed to have a role as an immune modulator. However, the association between vitamin D levels and anti-thyroid peroxidase positive (TPOAb) hypothyroidism is still controversial. Aim: To elucidate the association between vitamin D levels and anti-thyroid peroxidase (TPOAb) positive hypothyroidism. Materials and Methods: Serum Vitamin D, thyroid peroxidase antibody, and thyroid function test were measured in 105 patients, who were sub-grouped into the TPOAb positive and TPOAb negative hypothyroidism category. Results: Vitamin D level, was found significantly lower in patients with TPOAb positive hypothyroidism as compared to patients TPOAb negative hypothyroidism (13.27±5.18vs. 17.74±6.03ng/ml, respectively, P<0.05), as well as between patients with TPOAb positive hypothyroidism and control group (13.27±5.18vs. 29.66±9.41 ng/ml, respectively, P<0.05). Within the patients' group, there was a significant negative correlation between serum 25 (OH) vitamin D and TSH (r=−0.438, P<0.05), anti-TPO (r=−0.275, P<0.05). Furthermore, insignificant positive correlations were recorded between serum 25 (OH) vitamin D, and each of T3, T4 (r=–0.056, 0.097, P>0.05). Conclusion: The current study observed significant low levels of 25(OH)D3 in TPOAb positive hypothyroid patients.
Keywords: Vitamin D deficiency, anti-thyroid peroxidase antibody, autoimmune thyroiditis
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Professor, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India. Email:  |
Shankar M, Singh M. Is there any association between vitamin D deficiency and anti-thyroid peroxidase positive hypothyroidism: A cross-sectional study. Int J Med Res Rev. 2020;8(4):295-301. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1203 |
 |
 ©
©