Conformal radiotherapy plans for palliative bone metastasis - comparison of dosimetric parameters
Gupta N.1, Kumar P.2*, Kumar P.3, Navitha S.4, Mehta A.5, Chauhan A.6
DOI: https://doi.org/10.17511/ijmrr.2020.i03.02
1 Naina Gupta, Junior Resident, Department of Radiation Oncology, Shri Ram Murti Smarak Institute of Medical Sciences, Bareilly, Uttar Pradesh, India.
2* Pavan Kumar, Assistant Professor, Department of Radiation Oncology, Shri Ram Murti Smarak Institute of Medical Sciences, Bareilly, Uttar Pradesh, India.
3 Piyush Kumar, Professor and Head, Department of Radiation Oncology, Shri Ram Murti Smarak Institute of Medical Sciences, Bareilly, Uttar Pradesh, India.
4 Navitha S., Assistant Professor Cum Medical Physicist, Department of Radiation Oncology, Shri Ram Murti Smarak Institute of Medical Sciences, Bareilly, Uttar Pradesh, India.
5 Ankita Mehta, Junior Resident, Department of Radiation Oncology, Shri Ram Murti Smarak Institute of Medical Sciences, Bareilly, Uttar Pradesh, India.
6 Arvind Chauhan, Professor, Department of Radiation Oncology, Shri Ram Murti Smarak Institute of Medical Sciences, Bareilly, Uttar Pradesh, India.
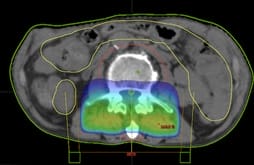
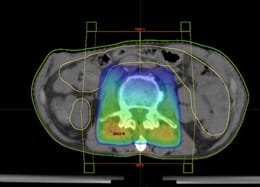
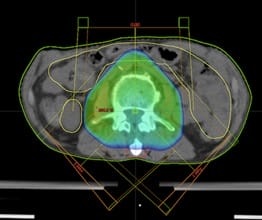
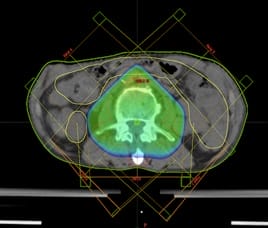
Background: Palliative radiotherapy offers significant relief in the huge physical distress of patients with bony metastasis. The enormous potential of conformal techniques has not been tested in palliative settings. However,the increasing life span of patients with metastatic disease demands to optimize the radiotherapy techniques to provide maximal durable symptomatic relief. Materials and Methods: Ten patients of vertebral bony metastasis were retrospectively selected and four virtual 3DCRT plans were generated for each patient. The field approaches were a single field, two fields, three fields and five field approaches. Results: A total of forty radiotherapy plans were generated. PTV parameters were significantly better with two field plans over one field plans in terms of D90 (p= 0.002), D50 (p= 0.02), Dmean(p=0.0009). Dmeanwassignificantly better with three field approach compared to two field approach (p=0.0006). Conclusion: The three field plans showed better dose distribution to the PTV with an acceptable increase in the dose to OAR’s.
Keywords: Conformal radiotherapy plans, Bone metastasis, Dosimetric parameters
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Radiation Oncology, Shri Ram Murti Smarak Institute of Medical Sciences, Bareilly, Uttar Pradesh, India. Email:  |
Gupta N, Kumar P, Kumar P, Navitha S, Mehta A, Chauhan A. Conformal radiotherapy plans for palliative bone metastasis - comparison of dosimetric parameters. Int J Med Res Rev. 2020;8(3):228-233. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1197 |
 |
 ©
©