A Case of Refractory Supraventricular Tachycardia in a Newborn
P.Wali P.1*, Khan A.2, Parakh H.3
DOI: https://doi.org/10.17511/ijmrr.2023.i01.04
1* Pradnya. P.Wali, MBBS, Dch,DNB Pediatrics, Fellowship in Neonatology, Shalini Hospital, Hyderabad, Telangana, India.
2 Aswad Khan, DNB Paediatrics, Fellowship in Neonatology, Consultant Neonatologist, Shalini Hospital, Hyderabad, Telangana, India.
3 Hemant Parakh, MD Paediatrics, DM Neonatology, Senior Consultant Neonatologist, Shalini Hospital, Hyderabad, Telangana, India.
Supraventricular Tachycardia (SVT) is the most common neonatal dysrhythmia with the incidence being 1 in 100 for children of all ages and 1 in 250 for neonates. The origin of supraventricular tachycardia is either above the bifurcation of the bundle of His or it has mechanisms dependent on the bundle of His. Newborns may present with irritability, poor feeding and tachypnea. The most important clinical sign of SVT is tachycardia sometimes associated with hypotension, heart failure, pallor, or decreased level of consciousness. Diagnosis is done with heart rate continuously remaining ≥ 220 beats per minute with a QRS < 0.08 seconds. Adenosine is the first-line abortive therapy of choice. Intractable SVTs are treated with amiodarone, esmolol, and procainamide. SVT with Circulatory collapse needs a synchronized DC cardioversion. Prognosis of SVT is generally excellent in the absence of structural heart disease.
Keywords: Neonatal tachyarrhythmia, Supraventricular tachycardia, Adenosine, Amiodarone, synchronized DC cardioversion
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Consultant Neonatologis, Department of Neonatology, Shalini Hospital, Hyderabad, Telangana, India. Email:  |
Pradnya. P.Wali, Aswad Khan, Hemant Parakh, A Case of Refractory Supraventricular Tachycardia in a Newborn. Int J Med Res Rev. 2023;11(1):22-27. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1193 |
 |
 ©
© 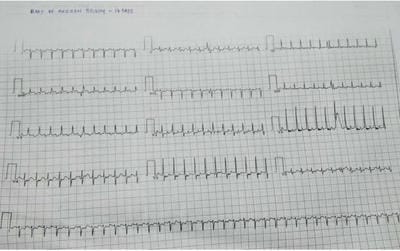 Figure 1: ECG showing Narrow Complex Tachycardia suggestive of SV
Figure 1: ECG showing Narrow Complex Tachycardia suggestive of SV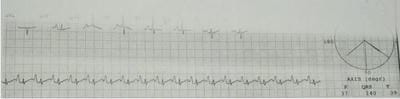 Figure 2: Resolution of SVT after Adenosine therapy.
Figure 2: Resolution of SVT after Adenosine therapy.