Isthmus agenesis with variant topography of levator glandulae thyroideae: A case report
Potaliya P.1*, Choudhary A.2, Ghatak S.3
DOI: https://doi.org/10.17511/ijmrr.2020.i03.10
1* Pushpa Potaliya, Assistant Professor, Department of Anatomy, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India.
2 Anju Choudhary, Senior Resident, Department of Anatomy, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India.
3 Surajit Ghatak, Professor and Head, Department of Anatomy, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India.
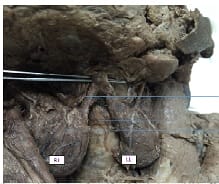
The thyroid gland is an imperative endocrine gland present in the neck known commonly for its morphological variations. During routine dissection agenesis of the isthmus of the thyroid gland was observed with levator glandulae thyroidea extending from both the lateral lobes with stout stalks of pyramidal lobes bilaterally. The Levator glandulae thyroidea is a fibro-musculo-glandular band. usually, present unilaterally or extending from isthmus connecting the pyramidal lobe of the thyroid gland to the hyoid bone. The site of the isthmus is often associated with anastomosis of vessels supplying thyroid gland but strikingly no such anastomosis was observed. The presence of such variant of levator glandulae thyroidea with agenesis of the isthmus is a rare finding and knowledge of such topographical anatomical variations is crucial for understanding associated pathologies related to the thyroid gland and modus operandi in their management.
Keywords: Anatomic variation, Thyroid gland, Anatomy, Isthmus, Agenesis
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Anatomy, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India. Email:  |
Potaliya P, Choudhary A, Ghatak S. Isthmus agenesis with variant topography of levator glandulae thyroideae: A case report. Int J Med Res Rev. 2020;8(3):273-276. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1192 |
 |
 ©
©