The paradigmatic shift in the clinical profile of dengue patients: a prospective observational study from a tertiary care center in north India
Lal Banthia B.1, Dubey P.2*, Arya S.3, Kumar Rao S.4
DOI: https://doi.org/10.17511/ijmrr.2020.i02.08
1 Bajrang Lal Banthia, Associate Professor, Department of Medicine, Teerthanker Mahaveer Medical College and Research Centre, Moradabad, Uttar Pradesh, India.
2* Prashant Dubey, Assistant Professor, Department of Medicine, Teerthanker Mahaveer Medical College and Research Centre, Moradabad, Uttar Pradesh, India.
3 Siddharth Arya, Junior Resident, Department of Medicine, Teerthanker Mahaveer Medical College and Research Centre, Moradabad, Uttar Pradesh, India.
4 Sandeep Kumar Rao, Junior Resident, Department of Medicine, Teerthanker Mahaveer Medical College and Research Centre, Moradabad, Uttar Pradesh, India.
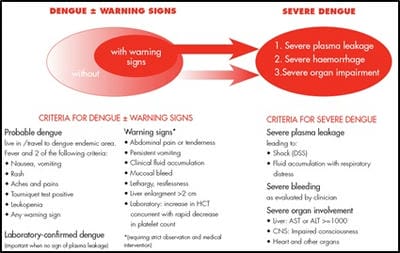
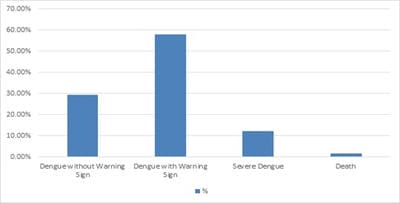
Background: Dengue a vector-borne viral disease transmitted by mosquito and has several complications causing fatalities and a bad impact on society. The paucity of studies in Uttar Pradesh and lack of epidemiological data necessitated to take up this prospective study. Purpose: The study is aimed at detecting clinical signs and symptoms of patients with dengue fever presenting to TMU teaching hospital between January 2019 to December 2019. Material and Methods: A prospective observational study was undertaken in serologically confirmed cases of dengue. The disease was analyzed for its clinical profile, required investigations were done and evaluated. Results: In the present study the clinical outcome was: 1) Dengue fever without warning sign was (29.46%). 2) Dengue fever with a warning sign (57.87%). 3) Severe dengue fever (12.12%). Mortality noted in the present study was 1.8%. Bleeding manifestations were noted in 8.2% of patients. Thrombocytopenia (<100,000) was noted in (85.85%) patients. Conclusions: Patients of dengue presented with fever, headache, myalgia, nausea, vomiting. Bleeding manifestations were looked for. Lab findings like leucopenia and deranged liver function test were more than other studies.
Keywords: Dengue fever, Severe dengue, Clinical profile
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Medicine, Teerthanker Mahaveer Medical College and Research Centre, Moradabad, Uttar Pradesh, India. Email:  |
Banthia BL, Dubey P, Arya S, Rao SK. The paradigmatic shift in the clinical profile of dengue patients: a prospective observational study from a tertiary care center in north India. Int J Med Res Rev. 2020;8(2):201-206. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1143 |
 |
 ©
©