A meta-analytic comparison of 8 methods of closed anterior shoulder dislocation reduction
Iqbalbhai Sadikot M.1, Samir Shah J.2*
DOI: https://doi.org/10.17511/ijmrr.2020.i02.12
1 Mariyam Iqbalbhai Sadikot, MBBS, AMC MET Medical College, Ahmedabad, Gujarat, India.
2* Jay Samir Shah, MBBS, AMC MET Medical College, Ahmedabad, Gujarat, India.
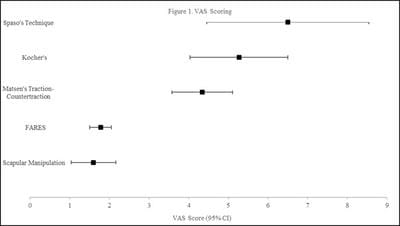
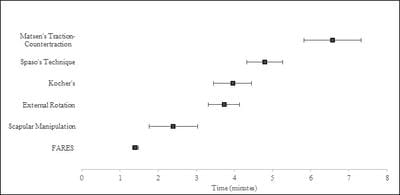
Background: Anterior shoulder dislocation is a common injury, accounting for 95% of all shoulder injuries. However, many doctors and hospitals do not have a fixed protocol for the treatment of dislocations. The current study have compared 8 different techniques for shoulder dislocation reduction in this study. Methods: Eight different methods namely the Scapular Manipulation, Matsen’s Traction-Countertraction, Kocher’s, Spaso, External Rotation, Cunningham, Modified Milch, and the FARES methods were compared on the basis of efficacy, pain experienced during reduction (VAS score), and time taken for reduction. Results: The Matsen’s Traction-Countertraction method had the highest efficacy, while the Scapular Manipulation method had the least VAS scoring. The FARES Method had the fastest reduction time on average. Interpretation and Conclusions: As per the data analyzed, the FARES and Scapular Manipulation method appear to be the most effective in reducing anterior dislocations, having consistently high success rates, and low VAS scores and reduction times. These 2 methods may be recommended to new practitioners to treat acute shoulder dislocations.
Keywords: Shoulder Dislocation, Emergency Medicine, Orthopedics
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , MBBS, AMC MET Medical College, Ahmedabad, Gujarat, India. Email:  |
Sadikot MI, Shah JS. A meta-analytic comparison of 8 methods of closed anterior shoulder dislocation reduction. Int J Med Res Rev. 2020;8(2):213-220. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1139 |
 |
 ©
©