Presentation of ischemic heart disease cases in tertiary care centres located in central India
Prakash Nayak O.1*
DOI: https://doi.org/10.17511/ijmrr.2019.i05.12
1* Om Prakash Nayak, Associate Professor, Department of Medicine, Chirayu Medical College & Hospital, Bhopal, Madhya Pradesh, India.
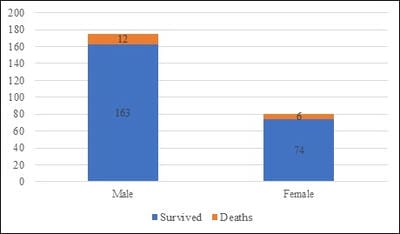
Background: Cardiovascular disease, one of the non-communicable diseases, has become a major public health problem in many developing countries. There is an epidemiological transition from infective/ communicable disease to Non communicable/degenerative diseases, increases in the prevalence of cardiovascular risk factors, and ageing of the population, which eventually leads to an increase in the absolute numbers of people with coronary heart disease (CHD) especially ischemic heart disease. This will need an increase demand of health awareness and demand for health care facilities. Aim: To know different ways of presentation of IHD cases. Material & Method: In this study total 255 IHD cases aged between 21 to 90 years were assessed between April 2017 to March 2018. Study was conducted in tertiary care centre located I central India. Informed consent was taken from patients or their relatives in case of unconsciousness of patient. Result: Total 255 patients were enrolled in this study out of which 175 were male with mean age of 58.57±7.2 years and 80 female patients were enrolled with mean age of 63.14±4.6 years. 18 patients were died. Most of the patients (59.22%) were mainly came with complain of chest pain. Other patients were coming with complain of breathlessness (7.06%), nausea/ vomiting (8.24%) and uneasiness (8.23%). Conclusion: over the time after independence trends and presentation of cardiovascular diseases especially ischemic heart disease is change. Knowing of current way of presentation is important. As disease trend is changing, knowledge of their pattern and availability of health resources accordingly is must.
Keywords: Cardiovascular disease, Ischemic heart disease, Coronary artery disease, Chest pain
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, Department of Medicine, Chirayu Medical College & Hospital, Bhopal, Madhya Pradesh, India. Email:  |
Nayak OP. Presentation of ischemic heart disease cases in tertiary care centres located in central India. Int J Med Res Rev. 2019;7(5):430-436. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1091 |
 |
 ©
©