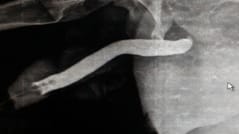
Sonourethrogram in comparison with retrograde urethrogram in evaluation of male anterior urethra
Haneef D.1*
DOI: https://doi.org/10.17511/ijmrr.2019.i05.07
1* D. Mahammad Haneef, Consultant Radiologist, Department of Radiology, Kurnool, Andhra Pradesh, India.
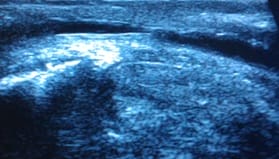
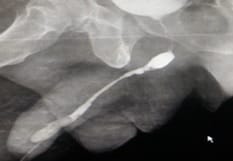
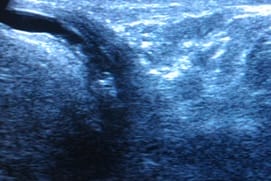
Objective: Imaging of anterior male urethra is usually done using retrograde urethrogram, which utilises radiation. This study utilises high resolution ultrasound which is radiation free and helps to understand urethral pathologies like strictures, chronic urethritis etc. This study also compares the utility of sonourethrogram with retrograde urethrogram and provides the advantages of using sonourethrogram. Also establishes the drawbacks of using sonourethrogram over retrograde urethrogram. Material & Methods: This study was done on 60 patients, came with different complaints like difficulty in micturition, obstructed urinary stream, pain in penis, increasing frequency of micturition and referred to us for retrograde urethrogram. Patients were examined with high resolution ultrasound with due permissions. Results are compared with findings of retrograde urerthrogram. Results: Out of 60 patients, 59 had strictures shown in retrograde urethrogram either in penile, bulbar or membranous parts. Only one patient had membranous urethral stricture in retrograde urethrogram which was not shown in sonourethrogram. All other patients have shown strictures in sonourethrogram. One patient had penile urethral calculus shown in both sonourethrogram and retrograde urethrogram. Conclusion: Sonourethrogram is equally effective as that of retrograde urethrogram especially in anterior urethral strictures. However, it underestimates or less useful in evaluation of posterior male urethral pathologies. Sonourethrogram is easily available, cost effective technique that uses no radiation in the evaluation of male urethra. It is equally effective compared to retrograde urethrogram in the evaluation of male anterior urethral strictures. Periurethral pathologies like fibrosis are better evaluated with sonourethrogram than with retrograde urethrogram. It is also important in the surgical planning and approach.
Keywords: Retrograde Urethrogram, Stricture, Sonourethrogram, Urethra
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Consultant Radiologist, Department of Radiology, Kurnool, Andhra Pradesh, India. Email:  |
Haneef DM. Sonourethrogram in comparison with retrograde urethrogram in evaluation of male anterior urethra. Int J Med Res Rev. 2019;7(5):389-395. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1084 |
 |
 ©
©