A morphometric study of adult human trachea in West Bengal population
Datta D.1, Kundu D.2*, Pal S.3, Das A.4
DOI: https://doi.org/10.17511/ijmrr.2019.i01.07
1 Dibyendu Datta, Medical Officer, Birpara State General Hospital, Alipurduar, West Bengal, India.
2* Dipankar Kundu, Associate Professor, Department of Biochemistry, Medical College, Kolkata, West Bengal, India.
3 Sharmila Pal, Professors & HOD, Department of Anatomy, Medical College, Kolkata, West Bengal, India.
4 Arijit Das, Tutor, Department of Pharmacology, Diamond Harbour Medical College, West Bengal, India.
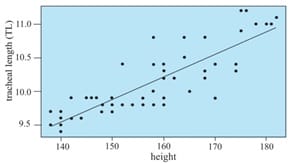
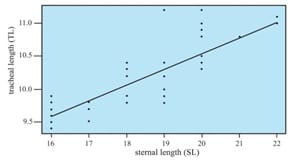
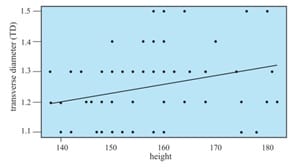
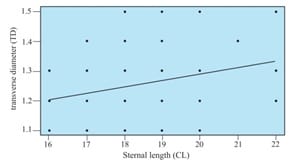
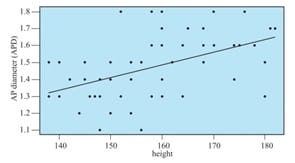
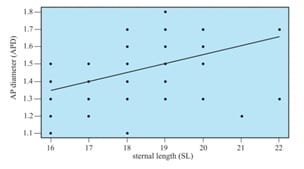
Background: Keeping in view the great variations in different dimensions of the human trachea and its remarkable clinical importance, the present work was undertaken. It included the study of dimensions of adult trachea of both sexes in West Bengal population. In addition, an effort was made to establish their relationship with selected external measurements. Methods: This was a cross-sectional, observational study on 60 cadavers. Relatively disease-free fresh adult cadavers were selected from West Bengal population. Study variables were tracheal length, internal transverse diameter and internal anteroposterior diameter. Selected external measurements were height and sternal length. Results: In males, the highest correlation was observed between tracheal length and height (r = 0.800), and tracheal length and sternal length (r = 0.799). In females, the highest correlation coefficient was found between tracheal length and height (r = 0.809). Conclusion: Different formulae were obtained by linear regression with all measurements being in centimeters. Therefore, it is possible to predict the tracheal dimensions from simple external measurements.
Keywords: Tracheal length, Internal transverse diameter, Internal anteroposterior diameter, Height, Sternal length
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, Department of Biochemistry, Medical College, Kolkata, West Bengal, India. Email:  |
Datta D, Kundu D, Pal S, Das A. A morphometric study of adult human trachea in West Bengal population. Int J Med Res Rev. 2019;7(1):36-42. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1033 |
 |
 ©
©